An Operating Model for Sustainable Healthcare Performance
Healthcare organizations are confronting a convergence of structural pressures that threaten the sustainability of traditional operating models. Fee-for-service margins continue to erode under payer rate pressure, labor and supply costs remain elevated, and public and private payers are accelerating the transfer of financial risk to providers while demanding measurable improvements in quality, outcomes, and patient experience. Transparency in performance reporting has further intensified scrutiny from regulators, employers, and consumers.
Over the past decade, many organizations responded by entering value-based contracts, launching pilots, or building care management programs. While these efforts often produced localized gains, most failed to deliver durable, enterprise-level transformation. Financial results were inconsistent, operational change remained fragmented, and improvements in clinical performance proved difficult to sustain.
Value-Based Enterprises (VBEs) represent the next stage of evolution. VBEs move beyond payment reform and care redesign toward a fully integrated enterprise operating model. They align governance, incentives, care delivery, and data infrastructure around defined populations and shared accountability for outcomes. Rather than layering value-based care on top of fee-for-service operations, VBEs redesign the organization itself to function under value-based economics
From Value-Based Payments to Value-Based Care to Value-Based Enterprises
Early value-based payment models introduced accountability without operational control. Shared savings arrangements, bundled payments, and upside-only risk contracts shifted financial exposure to providers while assuming capabilities that many organizations did not yet possess. As a result, providers bore risk without sufficient authority to manage utilization, variation, or total cost of care.
Value-based care emerged as a delivery response, emphasizing population health management, care coordination, and prevention. However, these efforts were often implemented as optional programs layered on top of fee-for-service structures. Lacking enterprise authority, they struggled to scale, enforce standards, or produce consistent financial results.
VBEs close this gap by aligning accountability with control. In a VBE, governance, decision rights, incentives, and data are aligned at the enterprise level, enabling repeatable performance under value-based economics across populations, service lines, and contracts.
Leadership self-assessment questions:
- Where do we currently accept financial accountability without operational authority?
- Which value-based initiatives remain optional or peripheral rather than embedded in core operations?
- Do governance and incentive structures reinforce enterprise performance—or preserve legacy silos?
Healthcare’s Non-Competitive Legacy
Healthcare’s current inflection point is the product of a historically non-competitive economic structure. Prices are largely set by insurers and government programs rather than market forces, weakening cost discipline and allowing inefficiency to persist. Patients are insulated from the true cost of care, blunting price sensitivity and limiting competition based on value.
In many markets, provider consolidation and regulatory barriers further reduce competitive pressure, while public policy has historically prioritized access and system stability over efficiency. Under fee-for-service economics, inefficiency was often tolerated or rewarded. Under value-based economics, it becomes a direct threat to margin and sustainability.
Why Value-Based Care Matters Now
Value-based care has shifted from experimentation to economic necessity. Medicare Advantage now dominates Medicare enrollment and operates under prospective, population-based payment. CMS has articulated a clear objective to place all Traditional Medicare beneficiaries into accountable care relationships by 2030.
As fixed budgets and public performance reporting replace volume as the primary financial driver, healthcare organizations increasingly compete on efficiency, outcomes, and experience. Those unable to manage risk at scale will face accelerating margin compression.
The Value-Based Enterprise Framework
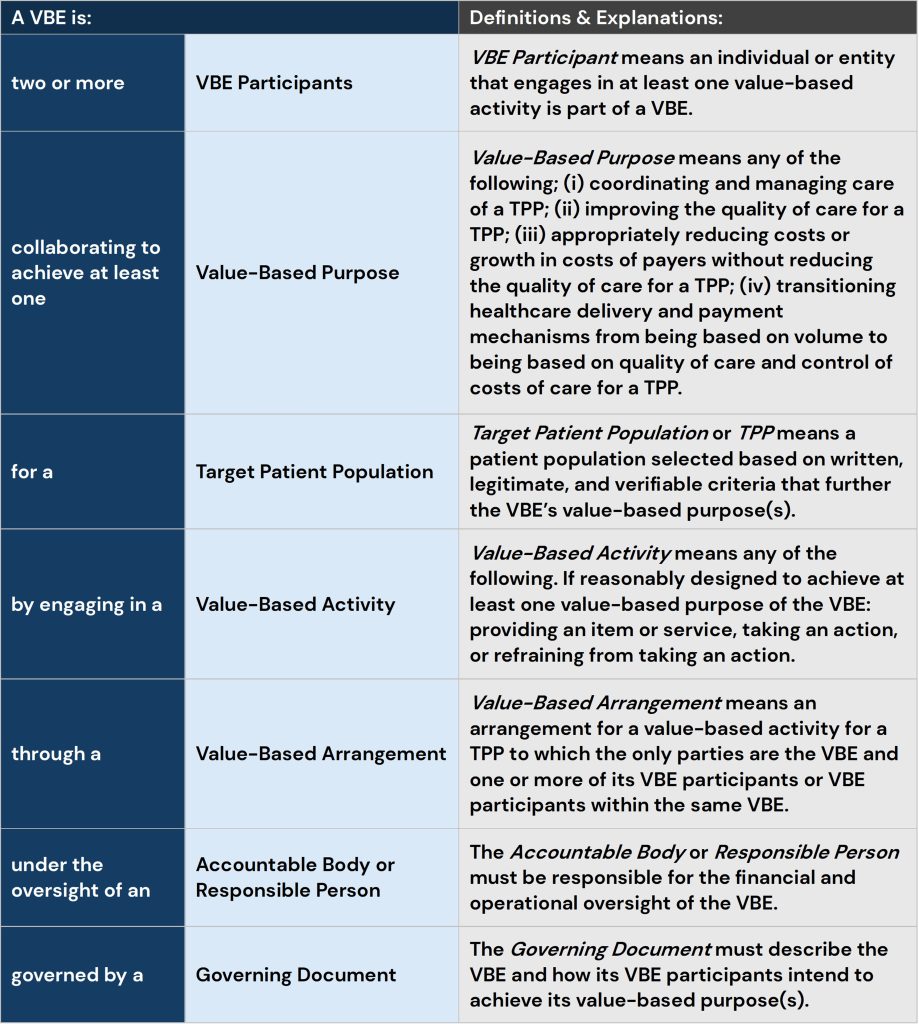
The Value-Based Enterprise framework provides the structural foundation for operating under value-based economics. A VBE consists of two or more participants collaborating to achieve defined value-based purposes for a clearly identified target patient population. These purposes include coordinating and managing care, improving quality, reducing cost growth without compromising quality, and transitioning delivery and payment from volume to value.
VBEs operate through value-based arrangements and activities governed by a formal structure that includes accountable oversight and documented governance. This framework enables organizations to align incentives, deploy resources flexibly, and operate within modern regulatory guardrails that support value-based care.
Leadership self-assessment questions:
- Can we clearly articulate our target patient populations and value-based purposes?
- Do our governing documents and decision rights support enterprise-level accountability?
- Are incentives explicitly tied to outcomes, efficiency, and quality—or implicitly tied to volume?
Regulatory Alignment and Incentive Design
Federal policy has evolved to support value-based care through updated fraud and abuse safe harbors and Stark Law exceptions. These frameworks allow greater flexibility in compensation, care coordination, and resource deployment when anchored to defined populations, articulated purposes, and accountable oversight.
Within VBEs, physician compensation evolves beyond pure productivity. Incentives reward participation in standardized care models, adherence to evidence-based pathways, and performance against quality and cost targets. Patient incentives reinforce preventive care, engagement, and adherence, aligning behavior across the ecosystem.
The Role of Primary Care and Specialists
Primary care serves as the foundation of value-based care through longitudinal relationships, risk stratification, and coordination across settings. Effective primary care reduces avoidable utilization and ensures continuity.
Specialists increasingly determine value-based performance. Specialty care drives a disproportionate share of spending and variation, particularly in episode-based models. Engaging specialists through tailored pathways, data transparency, and aligned incentives is essential to managing total cost of care.
VBEs integrate primary and specialty care through shared governance, aligned incentives, and common data infrastructure, enabling enterprise-level performance rather than siloed optimization.
Leadership self-assessment questions:
- Do specialists view value-based performance as core to their role—or as an external constraint?
- Where does unwarranted variation persist across specialty care?
- Are primary and specialty care aligned around shared outcomes and financial accountability?
The Transforming Episode Accountability Model (TEAM) as a Catalyst
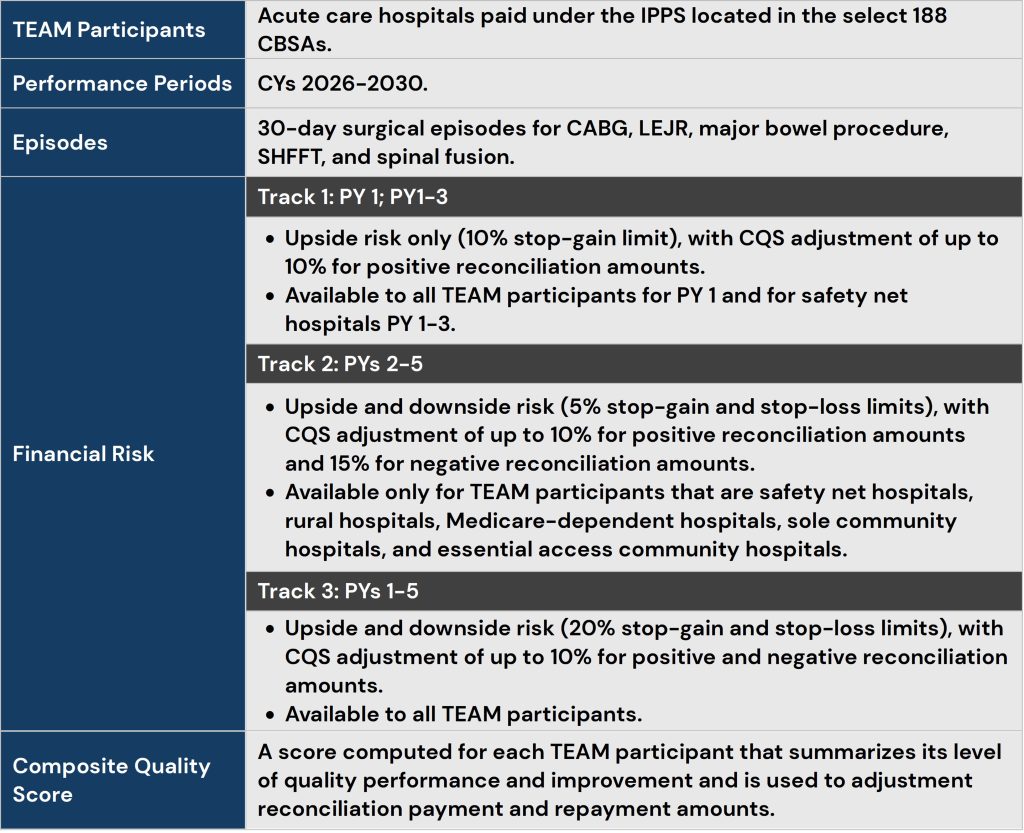
TEAM represents a significant acceleration of value-based accountability. Beginning in 2026, participating hospitals will assume responsibility for the cost and quality of defined surgical episodes across a 30-day window. Financial performance will be measured against target prices, with upside and downside risk tied to quality outcomes.
TEAM magnifies the need for enterprise coordination. Hospitals must actively manage care transitions, post-acute utilization, specialist behavior, and physician alignment. The scale and mandatory nature of TEAM make it a forcing function for adopting the VBE framework rather than relying on incremental or voluntary approaches.
What Fee-for-Service Organizations Must Address
Under value-based economics, characteristics once tolerated under fee-for-service become margin destroyers:
- Clinical Variation: Unwarranted variation directly erodes margins and quality.
- Care Leakage: Out-of-network utilization becomes a financial liability.
- Site-of-Care Inefficiency: High-cost settings undermine total cost performance.
- Misaligned Incentives: Productivity-only compensation conflicts with value-based goals.
- Diffuse Accountability: Delayed intervention increases financial exposure.
VBEs address these challenges through standardized pathways, managed networks, redesigned incentives, and clear enterprise accountability.
Financial Implications of Value-Based Enterprises
Value-based payment models do not inherently generate savings; execution quality determines outcomes. VBEs embed cost management into daily operations, creating durable financial performance through utilization management, site-of-care optimization, post-acute coordination, and quality improvement.
Aligned governance and incentives create compounding benefits, enabling predictable performance, stronger payer negotiations, and more strategic capital deployment. Conversely, weak execution under downside risk accelerates losses.
Leadership self-assessment questions:
- How quickly can we detect and intervene when cost or quality performance deviates?
- Are financial results driven by operational change or by favorable benchmarks and one-time effects?
- Does our balance sheet strategy reflect increasing exposure to downside risk?
Operationalizing Value-Based Enterprises Under TEAM
The shift to enterprise accountability becomes unavoidable under mandatory, episode-based risk models such as the Transforming Episode Accountability Model (TEAM). TEAM requires hospitals to assume responsibility for the cost and quality of defined surgical episodes across a 30-day post-discharge window, creating immediate exposure to variation, fragmentation, and post-acute inefficiency.
Under TEAM, hospitals remain paid under fee-for-service during the performance year, but retrospective reconciliation introduces meaningful upside and downside risk tied to total episode spending and quality performance. This structure magnifies the limitations of traditional operating models and accelerates the need for enterprise-wide coordination across physicians, post-acute providers, and ancillary services.
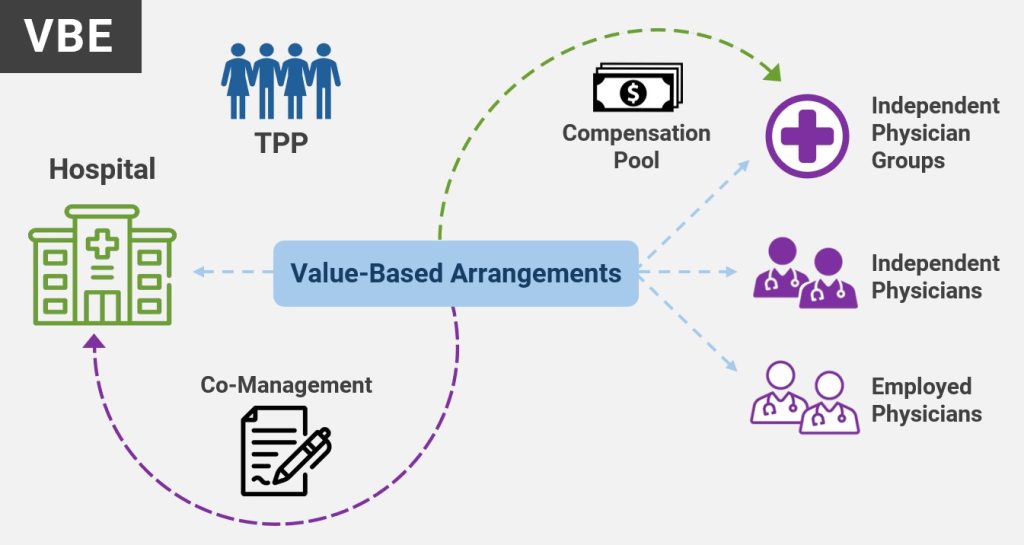
The Value-Based Enterprise framework provides a scalable mechanism for TEAM participants to align incentives, deploy resources, and manage risk across the full episode continuum. By forming a VBE, hospitals can engage physicians, post-acute providers, and other collaborators as VBE participants working toward shared value-based purposes for a defined target patient population. Within this framework, hospitals may deploy a wide range of value-based arrangements that are difficult or impossible to operationalize under traditional fraud and abuse exceptions. These arrangements include outcomes-based compensation, enablement, all tied to performance against cost and quality benchmarks.
Crucially, TEAM supplies much of the governance and accountability infrastructure required for a VBE. Participants already operate under defined episodes, articulated quality measures, and centralized financial accountability. When formalized through governing documents and accountable oversight, these elements allow TEAM participants to leverage value-based exceptions and safe harbors under the Stark Law and Anti-Kickback Statute, enabling broader and more flexible alignment strategies.
Expanding VBE Capabilities Across the Care Continuum
TEAM highlights that episode performance is not driven solely by hospital-based care. A significant portion of cost and variation occurs in physician decision-making and post-acute utilization. As a result, successful enterprises extend VBE arrangements across multiple points in the care continuum.
Hospitals may use VBE structures to support physician alignment through co-management and gainsharing arrangements that reward adherence to evidence-based protocols, operational stewardship, and episode efficiency rather than time-based services. These arrangements move beyond traditional medical directorships by granting physicians shared accountability—and, critically, shared authority—over care redesign, pathway standardization, and resource utilization.
VBE arrangements also enable hospitals to furnish in-kind support to independent physician groups, such as advanced practice providers, care coordinators, data analytics, and technology tools. These resources support pre-operative optimization, post-discharge follow-up, medication adherence, and complication prevention—key drivers of episode performance under TEAM.
Post-acute providers play an equally critical role. Through VBE participation, skilled nursing facilities, home health agencies, therapy providers, and other downstream partners can be integrated into standardized care pathways, data-sharing protocols, and performance-based financial arrangements. Aligning these providers around episode outcomes reduces readmissions, inappropriate utilization, and unnecessary length of stay.
As organizations mature, comprehensive VBEs can span primary care, specialty care, hospital services, and post-acute care, creating a unified operating platform capable of managing both episode-based and population-based risk.
Gainsharing and Co-Management as Enterprise Alignment Levers
Gainsharing and co-management are not tactical add-ons within a Value-Based Enterprise; they are foundational alignment levers that translate enterprise accountability into physician-level behavior change. When properly designed within a VBE framework, these mechanisms align clinical leadership, operational control, and financial incentives around shared outcomes.
Gainsharing enables organizations to reward physicians and care teams for achieving measurable improvements in cost, quality, and efficiency. Under a VBE, gainsharing pools can be tied directly to controllable drivers of performance—such as protocol adherence, length-of-stay reduction, post-acute utilization, and complication avoidance—rather than retrospective financial results alone.
Co-management arrangements extend beyond financial incentives to formalize shared governance. Physicians assume defined operational responsibilities for service-line performance, including pathway standardization, peer accountability, and continuous improvement. Compensation reflects outcomes and stewardship rather than volume or time-based effort.
Together, these tools allow enterprises to move from influence-based alignment to structurally embedded accountability, particularly in specialty care where variation and spend are most concentrated.
Leadership self-assessment questions:
- Where do we expect physicians to manage cost and variation without granting corresponding authority?
- Which service lines require co-management to achieve sustainable performance under risk?
- Are gainsharing and co-management deployed strategically, opportunistically, or at all?
Value-Based Enterprise Capability Maturity Model
Healthcare organizations typically progress through distinct stages as they evolve toward enterprise-level value-based performance. Understanding current maturity helps leaders sequence investments and manage risk deliberately.
Leadership self-assessment questions:
- Where does our organization truly operate today—not aspirational, but in practice?
- Which alignment mechanisms are missing at our current level of maturity?
- What capabilities must be built to progress to the next level of maturity?
- Are we sequencing transformation to match our risk exposure?
Conclusion: From Programs to Operating Model
Value-Based Enterprises represent a shift from episodic initiatives to a durable operating model. As mandatory and downside risk expands, organizations that align governance, incentives, and operations around value will be best positioned to compete.
The defining question is no longer whether value-based care will dominate healthcare economics, but whether organizations will mature fast enough to succeed under it.
If you have questions or for more information, please contact our strategy experts.


