Introduction
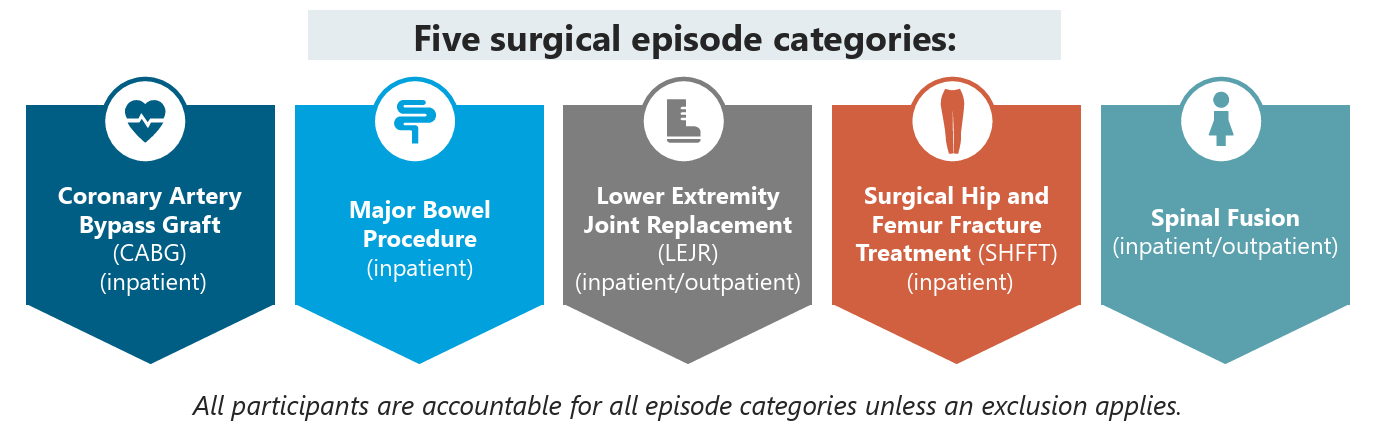
Under the Transforming Episode Accountability Model (TEAM), the cost of implants and instrumentation is included in a single, bundled payment for a surgical episode. There is no separate reimbursement for these items, which fundamentally changes how hospitals must manage costs and billing for high-cost implants.
CMS TEAM Internal Cost Savings vs. Medicare Spending Reductions
- Direct Savings (within Medicare’s fixed DRG reimbursement) negotiating lower implant prices to directly enhance hospital profitability, without reducing Medicare’s payments.
- Episode of Care Savings managing services such as SNF days, readmissions, and outpatient visits to reduce Medicare’s total episode costs. This will be crucial to achieving favorable reconciliation outcomes.
- Both types of cost control are required for success. Direct savings (lowering implant costs) to enhance profitability within Medicare’s fixed reimbursement, and episode of care cost reductions to secure program bonuses or avoid penalties during reconciliation.
Implications for Implant Costs
- Bundled payment: Under TEAM, Medicare provides a single target price that covers all services, items, and care related to a surgical episode. This shifts the financial accountability for the full episode of care to the hospital.
- No separate billing: Hospitals cannot bill separately for implants and other instrumentation used during a surgical procedure. All related supply and equipment costs must be managed within the fixed bundled payment.
- Reconciliation process: At the end of each performance year, CMS compares a hospital’s actual spending against its episode target price.
- If costs are below the target (and quality goals are met), the hospital may share in the savings.
- If costs are above the target, the hospital must repay the difference, which can be significantly impacted by the cost of implants.
- Focus on cost control: With implants bundled into the episode payment, hospitals are incentivized to control and manage supply costs more effectively. They must analyze their spending on a per-case basis and, for example, negotiate better prices with implant vendors to maximize financial success under TEAM.
- Mandatory participation: 741 acute care hospitals in selected Core Based Statistical Areas (CBSAs) were required to participate starting January 1, 2026. This represents about 10% of all hospitals.
Pinnacle’s primary focus is supporting implant cost reduction, cost avoidance, and clinical value analysis for CMS TEAM episodes with respect to LEJR, SHFFT and Spinal Fusion.
Below is an example TEAM episode with services offered over the episode of care. Pinnacle’s mission is to ensure a patient’s episode of care begins with favorable implant pricing with respect to the Hospital DRG Payment as a foundation for success.
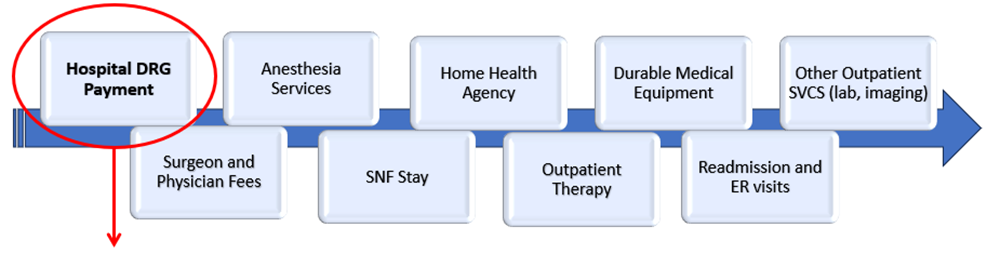
To accomplish this mission, the following outlines Pinnacle’s strategic support areas for TEAM focused data analytic and cost reduction as well as product line support for total joint replacement and spine fusions.
- Implant Categorization and Benchmarking
- Contracting
- Value Analysis Support
- OIG Gainshare Program Administrator
Implant Categorization/Cost Benchmarking
- Our team manages a proprietary database with an emphasis on implants supporting the Spine, Total Joints, and Cardiology service lines. The database contains over 550,000 unique items focusing primarily on physician preference items (PPI) such as biologics, implants (hardware), and instrumentation. Unique classifications are assigned to standardize the implants into clinically similar categories for focused analytics.
- Standardizing implants into clinically similar implant categories helps supply chain managers and administration better understand their implant formulary and utilization while creating a pathway to effectively communicate with surgeons.
- Pinnacle offers benchmarking to support the standardized implant clinical categories in order to help identify cost reduction opportunities.
Contracting
- The CMS TEAM program is a 5-year performance period. Because of the duration of the program, organizations and hospitals have incentive to assess PPI cost savings by reviewing and benchmarking current implant costs, and quickly identifying opportunities to secure favorable pricing that aligns with the TEAM model. Strategically, there are additional issues to consider, such as:
- Successfully navigating TEAM episodes will require surgeon engagement. Involving the surgeons in cost reduction efforts and facilitating dialog regarding contracting strategies will be critical.
- If your facility operates as an “all-play” model, are you looking to consolidate vendors?
- Are you actively recruiting surgeons?
- What are their vendor preferences, and do they use currently contracted vendors?
- Do they frequently utilize higher cost assemblies or implants?
- To what degree will surgeons support a cost savings initiative?
- Is there consideration of a gainshare program to promote surgeon engagement?
- Along with contracting, TEAM participants should implement auditing strategies to assure contract compliance with pricing and purchase agreement terms and conditions.
Value Analysis Support
- Our consultants help to alleviate capacity constraints caused by staffing shortages, adding value by providing supply chain teams with dedicated expertise and clinical insights.
- Provide or develop value analysis documents unique to each facility to assist in the review of new product requests by surgeons/vendors.
- Support the value analysis team including financial review of new products.
OIG Gainshare Program Administrator
- Our physician preference item focused supply chain team has successfully developed, deployed, and administered OIG compliant gainshare programs nationally. These programs continue to be a successful cost reduction strategy with additional benefits including increased surgeon engagement and communication.
- Components of an OIG compliant gainshare:
- Provide guidance and supporting documentation explaining the program, address questions, and facilitate discussion between surgeons and hospital administrators
- Savings assessment
- Implementation including tracking savings and case audits
- Monthly reporting
- Custom reporting and surgeon profiles
Expertise That Enhances Results
- We have assembled a team of experts who help clients filter the noise during negotiations and discussions concerning high-cost implants and physician preference items. We currently participate in materials management discussion as a clinical liaison between vendors, supply chain managers, and surgeons. For example:
- Supply chain will frequently engage surgeons in conversations regarding spinal implants. The hospital data describing these implants is typically high level. For instance, there are many types of screws that may make up a broad “spinal screw” category. When surgeons are engaged to discuss cost and/or utilization metrics they are looking for the discussion to flow into clinical categorizations for a spine screw, such as “cervical screw”, “pedicle screw”, or “lumbar screw”. All are distinctly unique and pricing and clinical use is not comparable. Not knowing the differences and clinical nuances of the implants can erode the surgeon’s confidence and participation in discussions.
- Hospital administration may look at cases from a DRG perspective which can distort cost per case variances when comparing surgeons. For example, Cervical Fusions will typically fall under DRG’s 471, 472, or 473. However, the implant supplies can vary significantly as these DRGs describe cases that can either be one level or multi-level cases. If one surgeon performs mostly 1 level cases while another performs primarily 2 or 3 level cases, supply costs will vary significantly between the surgeons yet fall under the same DRG. Acknowledging these nuances in cost reduction discussions is critical to establishing surgeon confidence and support with supply chain administrators and cost reduction efforts.
- Total Joints: Vendors are constantly updating their implant offerings requiring addendums and formulary maintenance for the duration of a purchase agreement. In many instances they will request implant pricing exceptions and/or implant designations that are out of alignment with a facilities purchase agreement language and pricing structure. Recently, several vendors have introduced implants targeted at patients who may have a nickel sensitivity. While these implants are “new” to those vendors, there are common implants and assemblies available that address this niche. Our implant team will help assess this type of request and work with the supply chain team to determine:
- Does the facility currently have nickel sensitive assemblies on formulary? If so, that can be used as a cost baseline in negotiating pricing.
- Have surgeon(s) specifically asked for these implants, or is the vendor requesting the addition?
- Are there unique attributes of the implants where a pricing exception should be considered?
- Are there clinical protocols in place for identifying nickel sensitive patients? Essentially, matching the correct implants as nickel sensitive assemblies or components can add additional costs.
Conclusion
The Transforming Episode Accountability Model (TEAM) represents a structural shift in how surgical episodes are financed, managed, and reconciled. By embedding implant and instrumentation costs within a single, predetermined bundled payment, CMS has effectively transferred full financial accountability for physician preference items (PPI) and post-acute performance to participating hospitals
Under TEAM, implant strategy is no longer a supply chain issue alone, and has become a margin protection and risk management imperative. Internal cost control (e.g., implant price optimization within a fixed DRG payment) enhances hospital profitability. External cost management (e.g., reducing readmissions, SNF utilization, and outpatient leakage) determines reconciliation outcomes and bonus eligibility. Sustainable success requires disciplined execution on both fronts.
Hospitals that treat implant categorization, benchmarking, surgeon engagement, contracting rigor, and gainshare alignment as foundational strategies will be best positioned to perform favorably during annual reconciliation. Those that do not will find that even modest implant cost variances can materially impact repayment exposure.
Ultimately, the margin in TEAM will be won or lost at the case level. Precision in data, precision in contracting, and precision in clinical alignment.
Call to Action
With mandatory participation underway across 741 hospitals, the time for preparation has passed, and execution is now a required imperative.
Hospitals participating in TEAM should immediately:
- Conduct a comprehensive implant categorization and benchmarking review
- Assess contract compliance and pricing alignment across high-volume service lines (LEJR, SHFFT, Spinal Fusion)
- Engage surgeons in structured cost discussions supported by clinically granular data
- Evaluate the feasibility of an OIG-compliant gainshare program
- Establish ongoing auditing and reporting mechanisms to monitor case-level performance
TEAM is a five-year performance model, so early structural optimization compounds over time.
Organizations that build a disciplined implant governance framework now will protect margin, strengthen surgeon alignment, and position themselves to earn rather than repay reconciliation dollars.
The question is no longer whether TEAM will impact financial performance. The question is whether your organization is positioned to win under it. If you have questions or would like to discuss your TEAM strategy, please reach out to have a discussion with our experts at Pinnacle Healthcare Consulting.
Resources
https://www.cms.gov/files/document/team-overview-updated.pdf

